|
INTRODUCTIONThe goals of therapy for type 2 diabetes are to prevent or delay complications and maintain quality of life. This requires control of glycaemia, management of cardiovascular risk factors, regular follow-up and importantly a patient-centred approach.1 This is in line with the Nursing and Midwifery Council (NMC) Code, which says that nurses should ‘prioritise people, practise effectively, preserve safety and promote professionalism and trust’.2 In addition, National Institute for Health and Care Excellence (NICE) guidelines emphasise the importance of taking into account individual needs and preferences.3LEARNING OBJECTIVESOn completion of this module, you will:
This module is one of a series of five. Others in the series are:
This resource is provided at an intermediate level. Read the article and answer the self-assessment questions, and reflect on what you have learned. Complete the resource to obtain a certificate to include in your revalidation portfolio. You should record the time spent on this resource in your CPD log. Individualised care in type 2 diabetes: involving patientsProviding patient-centred care that is responsive to individual patient preferences is essential for effective management of type 2 diabetes.1 Successful management involves shared decision-making, where the healthcare professional acknowledges the patient’s views about their condition and its treatment.4 All patients should be offered the opportunity to be involved in making decisions about the medicines they are prescribed.4 A patient-centred approach encourages informed adherence to medication.4 Poor adherence to therapy affects almost half of people with diabetes, leading to suboptimal glycaemic and cardiovascular risk factor control, and increased risk of complications and mortality, as well as higher long-term health care costs.1 Consider the individual patient’s circumstances, other illnesses and risk factors when agreeing targets. The NICE guideline on the management of type 2 diabetes recommends an HBA1c target of between 48 mmol/mol and 53 mmol/mol,3 but suggests that the healthcare professional should consider relaxing the target HbA1c level (on a case-by-case basis) for individuals:
When caring for older adults with type 2 diabetes, particular consideration should be given to their broader health and social care needs. Older people are more likely to have co-existing conditions and to be taking a higher number of medicines than younger patients. Their ability to benefit from risk-reduction in the longer term may also be reduced.3 Clinical characteristicsWhen selecting which agent to use to control blood glucose, it is important to consider the patient’s clinical characteristics very early in the process of treatment selection.1 These include a history of cardiovascular disease (CVD), renal impairment, weight, hypoglycaemic risk, and the patient’s age.1 The American Diabetes Association/European Association for the Study of Diabetes (ADA/EASD) 2018 consensus statement on the management of type 2 diabetes, states that evidence from cardiovascular outcome trials (CVOTs) shows compelling evidence for the benefits of specific medications – SGLT2 inhibitors and GLP-1 RAs – to reduce mortality, hospitalisation for heart failure (HF), and progression of renal disease in the setting of type 2 diabetes and established CVD.1 This was reinforced in the 2019 update, which states that these agents should be used not only in patients with CVD, but also without established CVD but with indicators of high risk.5 ADA/EASD5 (2019) recommends:
NICE acknowledges that the role of clinical characteristics is particularly important in informing the choice of medication at first intensification (after metformin plus lifestyle advice).3 The February 2022 guideline update states that patients' cardiovascular status and risk should be assessed, to determine whether they have HF or established atherosclerotic disease, or are at high risk of developing CVD. If they have HF, or established CVD, they should be offered an SGLT2 inhibitor (with proven cardiovascular benefit), in addition to metformin. If they are at high risk of developing CVD, consider an SGLT2 inhibitor (with proven cardiovascular benefit, in addition to metformin.3 NICE only recommends treatment with a GLP-1 RA if triple therapy with metformin and two other oral drugs is not effective, not tolerated or contraindicated. NICE recommends switching one oral drug for GLP-1 RA for adults with type 2 diabetes, who:
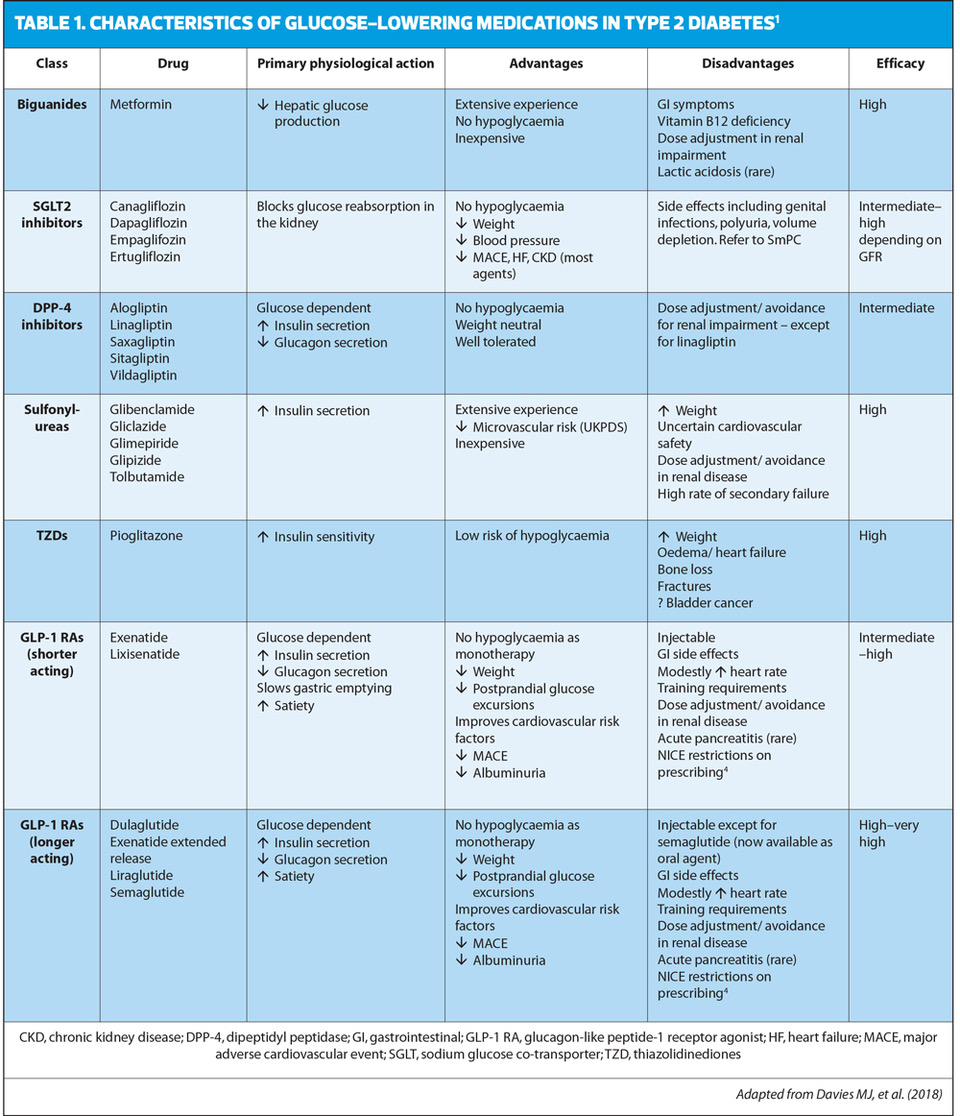
Choice of agentThe management of hyperglycaemia in type 2 diabetes has become increasingly complex with the number of glucose-lowering medications now available,1 and while this enables general practice nurses to offer a wider choice of therapeutic options, it can also pose challenges in terms of keeping up to date and understanding the advantages and disadvantages of each drug. When considering which drug is appropriate for the individual with type 2 diabetes, thought should be given to the mode of action, any side effects, any impact on renal function, potential effect on cardiovascular risk, and the cost of the drug. Before prescribing any drug, it is important to check the summary of product characteristics (SmPC) for any warnings or cautions, as well as for recommended dose. The following table summarises the main characteristics of each class.
The NMC CodeGeneral practice nurses do not need to be experts in diabetes to be able to understand the key indications for the drugs used in its treatment, and to understand when drugs may not be recommended or simply less suitable for the individual patient. People should be given the opportunity to discuss the effects and side effects of the range of therapies available. Even when the nurse is not the prescriber, she or he is the patient’s advocate, and each nurse has a duty to practise according to the NMC’s ‘4Ps’:
Ensuring that people with diabetes have tailored treatment that optimises outcomes and minimises risks will help you to meet these requirements. In the self-assessment that follows, hypothetical case scenarios based on fictitious patients are presented. Please refer to the relevant Summary of Product Characteristics before prescribing any of the medications mentioned.
References1. Davies MJ, D’Alessio DA, Fradkin F, et al. Management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2018;41:2669-2701 2. Nursing and Midwifery Council. The Code: Professional standards and behaviours for nurses and midwives, 2015. https://www.nmc-uk.org/standards/code [Accessed June 2022] 3. NICE NG28. Type 2 diabetes in adults: management, 2015 (updated 2022) https://www.nice.org.uk/guidance/ng28 [Accessed June 2022] 4. NICE CG76. Medicines adherence: involving patients in decisions about prescribed medicines and supporting adherence; 2009 (Reviewed March 2019). https://www.nice.org.uk/guidance/cg76 [Accessed June 2022] 5. Buse JB, Wexler DJ, Tsapas A, et al. 2019 update to: Management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2020;43(2):487-493
|
|